How 8-Hour Desk Jobs Are Spiking Cholesterol in Karachi's Professionals

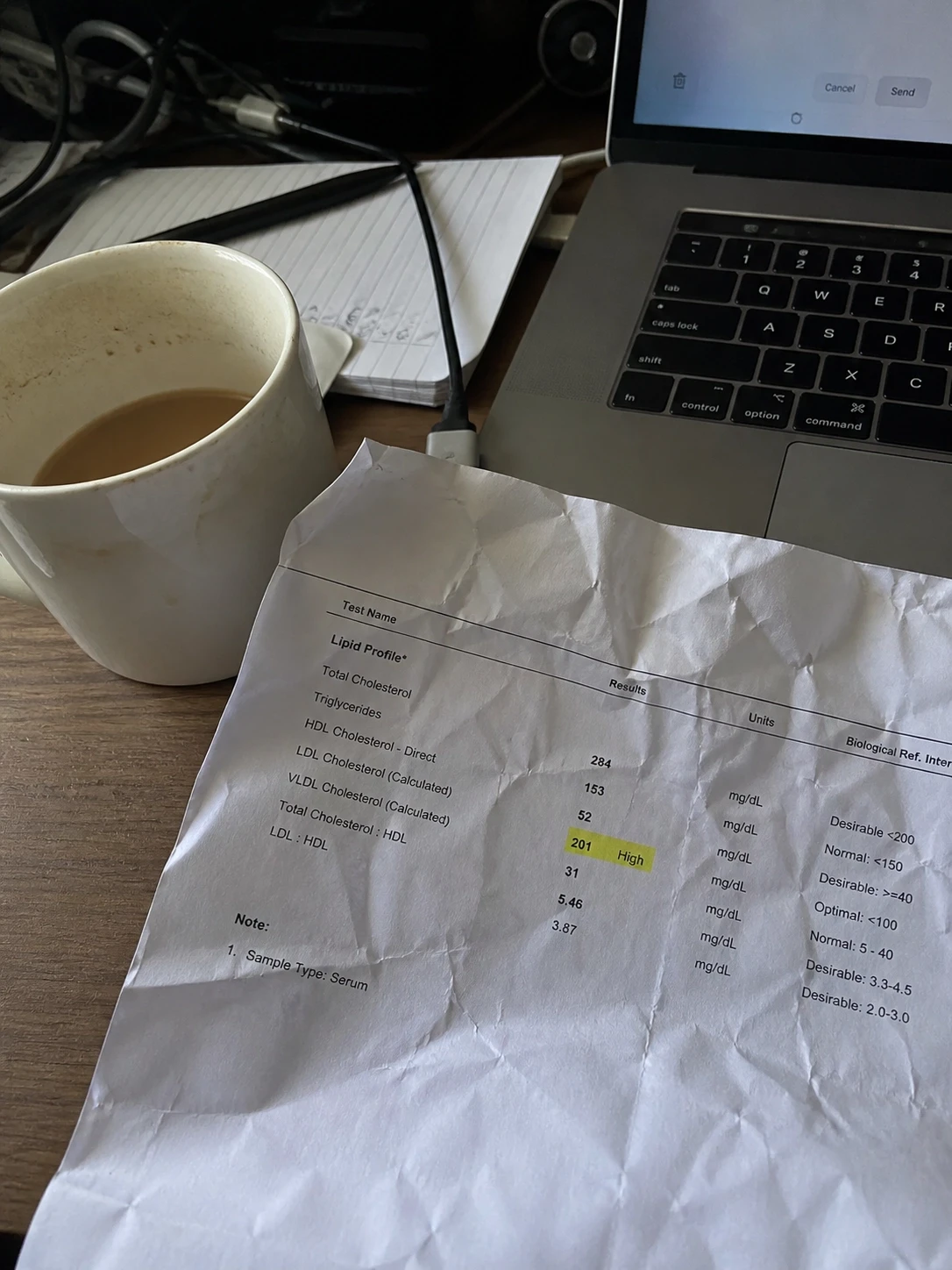
I see it every week. A 33-year-old banker sits across my desk, lipid profile in hand, visibly confused. LDL-C at 168 mg/dL. Triglycerides nudging 220. HDL so low that it is hardly considered protective. In six months he has not had a burger. He takes the stairs. He doesn’t smoke. He actually does not know what is wrong with his arteries, why they are acting like those of a 52-year-old with a lifelong junk food habit. This is the new normal in the corporate corridors of Karachi, and most professionals are not aware of this until the damage is done.
The first thing I tell every patient is that sitting is not passive. It is an active metabolic insult to your cardiovascular system. According to research published in the Circulation (American Heart Association), South Asians develop coronary artery disease 5 to 10 years earlier than Western populations - and carry a disproportionately higher risk of fatal cardiac events at every age bracket. That is not a scare statistic. That is your biological reality.
Add to that the nature of your workday - eight, nine, sometimes eleven hours anchored to a chair - and you have created the ideal conditions for what cardiologists increasingly call "sitting disease." A condition with no symptoms, no warning, and a potentially catastrophic endpoint. If you are a professional in Karachi between the ages of 28 and 45 and you have not had a preventative health screening Karachi, this article is for you.
What Your Office Habits Are Doing to Your Arteries
The Office Habit | The Metabolic Reality (With Stat) | The Medical Consequence |
Sitting uninterrupted for 3+ hours | Lipoprotein lipase (LPL) activity drops by up to 90% within 1 hour of muscular inactivity. Fat-clearing in the bloodstream effectively halts. | Rapid LDL-C and triglyceride accumulation; accelerated plaque formation in coronary arteries |
The 4 PM chai and biscuit spike | Refined carbohydrates consumed while seated trigger insulin surges that redirect dietary fat into storage rather than oxidation. Triglycerides can spike 20–30% above fasting baseline within 2 hours. | Postprandial hyperlipidemia; sustained elevated TG levels over time directly linked to atherosclerotic progression |
Assuming a thin body means healthy arteries | South Asians carry significantly higher visceral adiposity at lower BMI levels. A 2021 published research on South Asian visceral adiposity found South Asian adults have a higher metabolic risk burden than white adults at the same BMI - a phenomenon clinicians call TOFI (Thin Outside, Fat Inside). | Undiagnosed dyslipidemia; elevated cardiovascular event risk despite normal body weight |
The Biochemistry of the Desk Chair
Your chair is not a neutral object. Every hour you spend in it without moving is an hour your body spends dismantling its own defenses against cardiovascular disease. Here is exactly what is happening inside you right now.
1. The Enzyme Shutdown: What Sitting Does to Lipoprotein Lipase
Lipoprotein lipase (LPL) is the enzyme responsible for breaking down triglycerides - the fat particles circulating in your blood - so they can be burned as energy by your muscles. It is your body’s primary fat-clearing mechanism. And it is controlled almost entirely by muscular contraction.
When your leg muscles are active, LPL output is high. Blood fats are cleared. When your legs are motionless - as they are for eight hours across your desk - LPL activity collapses by up to 90% within the first hour. This was demonstrated conclusively in a foundational study by Bey and Hamilton, published in the Journal of Physiology. The moment you sit down, fat clearance virtually stops. Triglycerides accumulate. The number and density of the LDL particles increase. HDL - the protective cholesterol that scavenges arterial plaque - begins to fall.
By the time you finish your evening meeting and reach for your keys, your blood lipid profile looks measurably worse than it did at 9 AM when you arrived. Not because of what you ate. Because of what you did not do.

2. The South Asian Phenotype: Why Being 'Skinny' in Karachi Doesn't Protect You
This is the argument I hear most often and it frustrates me every time: "But doctor, I am not overweight." Weight is irrelevant if you are South Asian.
The TOFI phenotype - Thin Outside, Fat Inside - is disproportionately prevalent in our population. South Asians accumulate visceral adipose tissue (fat around and inside the organs) at significantly lower BMI thresholds than other ethnicities. This visceral fat is metabolically toxic. It releases inflammatory cytokines, drives insulin resistance, suppresses HDL production, and elevates LDL-C and triglycerides - all while your bathroom scale tells you everything is fine.
A landmark analysis confirmed that South Asian adults carry a substantially higher metabolic risk burden than white European adults at equivalent BMI values. The American Heart Association’s Circulation has flagged South Asian ethnicity as an independent risk factor for premature atherosclerotic cardiovascular disease - not because of diet alone, but because of our genetic predisposition to dyslipidemia and insulin resistance. A low-normal BMI does not neutralise that.
3. The "Active Couch Potato" Illusion: Why Your Evening Gym Session Is Not Enough
Your 45-minute gym session at 7 PM does not cancel out 9 hours of dead, uninterrupted sitting. You cannot out-train a biologically stagnant workday. Your enzymes have already shut down.
This is the Active Couch Potato paradox - and it is backed by substantial research. A study published in Scientific Reports found that even among individuals who met the recommended weekly physical activity targets, prolonged uninterrupted sitting was independently associated with adverse lipid profiles and elevated cardiometabolic risk. The exercise didn’t undo the damage. It simply coexisted with it.
The biology is unforgiving here. LPL suppression occurs in real time, hour by hour, proportional to muscular inactivity. An intense 45-minute bout cannot retroactively reverse nine hours of enzymatic shutdown. The metabolic insult is cumulative, not compensatory.
4. The Triglyceride Trap: Stress, Sitting, and the 4 PM Office Carb
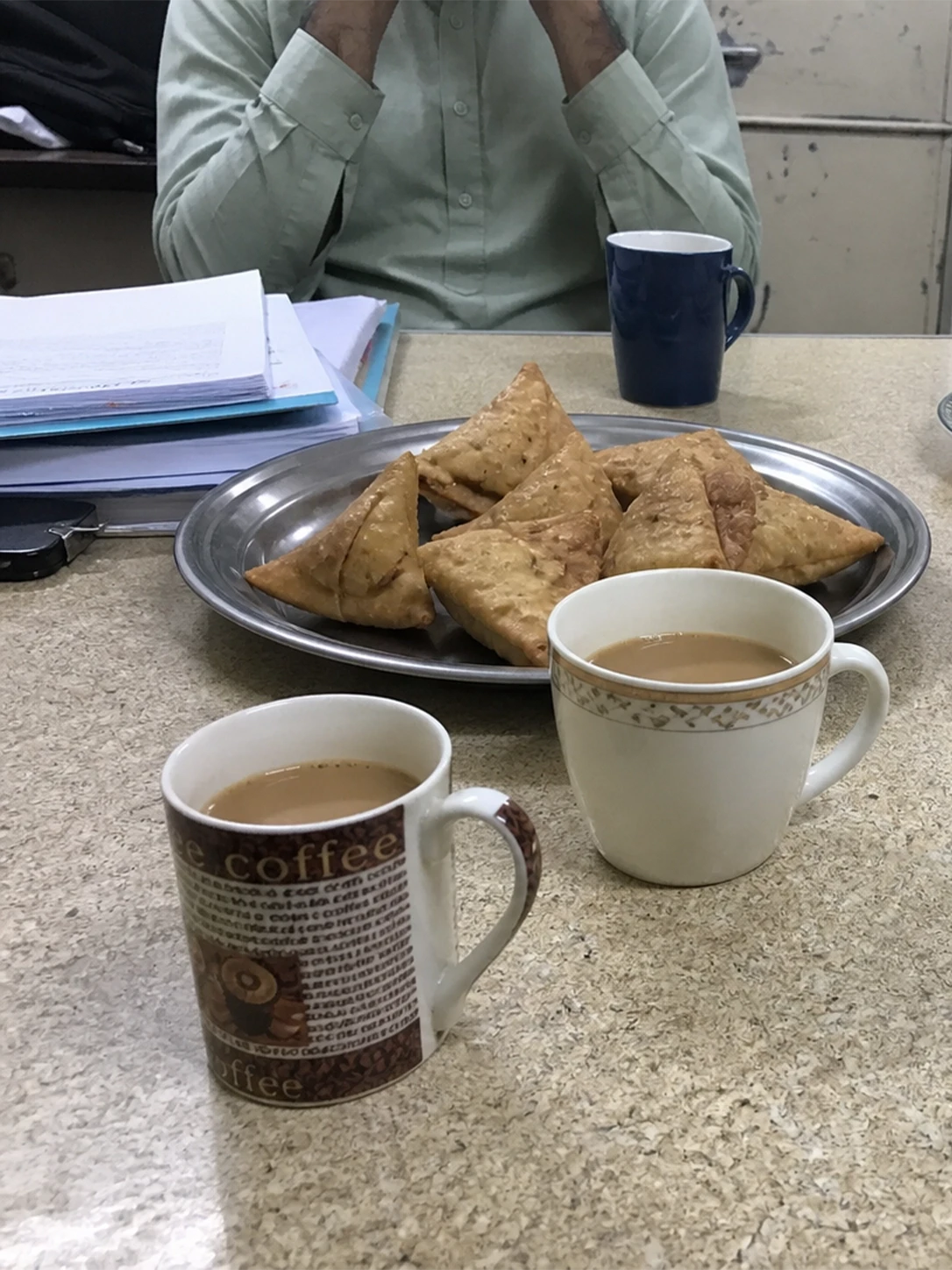
Let's talk about the 4 PM influx. You know exactly what I mean: the office boy materialises with a tray of oily samosas, a platter of biscuits, and glasses of heavily sweetened chai. It is not a snack. It is a metabolic ambush.
Refined carbohydrates consumed by a body that has been sedentary for six hours are handled entirely differently than carbohydrates consumed by an active one. With LPL activity already suppressed, there is no muscular fuel demand. Insulin spikes sharply. The liver converts the glucose surplus into triglycerides and packages them into VLDL particles that enter the bloodstream. Triglyceride levels can climb 20–30% above fasting baseline within two hours of a high-glycaemic meal taken at rest.
Now layer cortisol on top of that. Chronic work stress - the kind endemic to Karachi’s banking and tech sectors - elevates cortisol, which stimulates hepatic lipogenesis (liver-based fat production) and further increases VLDL output. The result is a triple assault: sedentary suppression of fat clearance, postprandial triglyceride flooding, and stress-driven hepatic lipid overproduction. This is the exact biochemical environment in which atherosclerotic plaque accelerates.
5. The AI Paradox: Smarter Tools, Stiller Bodies
Here is the part no one in your IT department's wellness newsletter will tell you. The very AI tools that are causing you to be more productive are also causing you to be more sedentary - and your arteries are paying the price.
ChatGPT, Microsoft Copilot, Gemini, and their counterparts have fundamentally changed the texture of a white-collar workday. Tasks that previously required walking to a colleague’s desk, attending a brief meeting, or physically retrieving a document - micro-movements that cumulatively added up to hundreds of muscle contractions per day - are now resolved in seconds from a single chat interface. This was explicitly flagged in a 2025 report from the International Labour Organization: AI-driven, algorithmically managed work environments are deepening sedentary exposure in desk-based roles, with workers increasingly anchored to a single screen for longer uninterrupted stretches.
Consider what AI actually eliminates from your day. The walk to a printer. The trip to a colleague for a second opinion. The physical search through a document folder. The informal stand-up at someone else’s workstation. These were not just social rituals. Each was a micro-interruption of sedentary time - the exact mechanism that partially restores LPL activity. Strip them away through automation and you have compressed nine hours of desk time into nine hours of almost unbroken sitting. A 2025 SITFLEX accelerometer study measuring desk-based workers across multiple environments found that sedentary bouts are longest and daily step counts lowest in the most digitally integrated work settings - including remote-work configurations where AI tool usage is highest.
McKinsey data from 2025 reports that 91% of employees now work in organisations that deploy at least one AI productivity tool. For Karachi’s banking and technology professionals - already among the most sedentary occupational groups - this means the metabolic floor has dropped further. The 8-hour desk job is becoming a 9-hour chair sentence, and the LPL enzyme suppression that begins within the first hour does not care how intelligent the software running on your screen is.
AI is not the villain here. But efficiency without movement is not health. If your AI tools are saving you two hours of task time per day, those two hours are almost certainly being spent seated. The productivity gain is real. The metabolic cost is also real. And unlike your quarterly KPIs, your lipid profile does not reset at the end of the financial year.
The 'Silent Symptoms' Reality Check: Why Waiting Is Dangerous
Here is what high cholesterol does not do: it does not give you warning signs. There is no pain, no fever, no indicator that sends you to a doctor. Atherosclerotic plaque accumulates in complete biological silence.
High LDL-C and triglycerides produce zero physical symptoms until a cardiac event - a myocardial infarction or stroke - occurs. The first symptom of undetected dyslipidemia is often the last one.
The dangerous cultural assumption that ‘I feel fine, so I am fine’ has no metabolic basis whatsoever. Coronary artery disease can be 70% occlusive before a single symptom appears.
That heavy, sluggish feeling in your calves by 3 PM - the pooling sensation, the legs that feel like they need to be stretched - is your circulatory system signalling venous stasis. It is not tiredness. It is physiology.
Chronic afternoon brain fog is frequently not a sleep deficit. It is a metabolic signal. Impaired postprandial lipid clearance and transient drops in cerebral perfusion - caused by elevated blood viscosity from high triglycerides - produce exactly that heavy, unfocused mental state you are attributing to your late nights.
If you are relying on a corporate health doctor consultation only when you feel sick, you are already operating on the wrong timeline.
Rapid-Fire Clinical FAQs
How does sitting all day affect my cholesterol and lipid profile?
Sustained sedentary behaviour directly suppresses lipoprotein lipase, the enzyme responsible for clearing triglycerides from your blood. Research shows LPL activity can fall by up to 90% within one hour of muscular inactivity (Bey & Hamilton, Journal of Physiology, 2003). This results in measurable increases in LDL-C and triglycerides and a corresponding decline in HDL-C over weeks and months of repeated sedentary exposure - even in the absence of dietary changes.
Can I lower my cholesterol if I have a desk job?
Yes, but it requires addressing the interruption of sitting, not just adding exercise. Micro-movement breaks every 30–45 minutes - even a two-minute walk to a colleague’s desk - partially restore LPL activity and blunt postprandial triglyceride spikes. Standing desks, combined with genuine ambulatory movement throughout the day, have shown measurable improvements in lipid profiles in occupational health trials. Dietary shifts toward lower glycaemic index foods - particularly at the 4 PM break - reduce the triglyceride load on a system already compromised by inactivity.
How often should desk workers in their 30s get a lipid profile?
The clinical standard for adults in their 30s with no known cardiovascular risk factors is a fasting lipid panel every four to five years. However, for South Asian professionals - particularly those in sedentary roles, under chronic occupational stress, or with a family history of premature cardiac disease - I recommend annual lipid profiling from the age of 28. For those already showing borderline results, a repeat panel every six months is appropriate
Is using AI tools at work making my cholesterol worse?
Indirectly, yes - and this is a question I am increasingly hearing in 2025 and 2026. AI productivity tools eliminate many of the small physical interruptions that previously punctuated a desk job: the walk to a printer, the brief stand-up at a colleague’s workstation, the physical search through a filing system. Each of those micro-movements was partially restoring LPL activity throughout the day. A 2025 ILO report on AI and occupational health identified deepening sedentary exposure in AI-managed work environments as an emerging occupational health risk. If your AI tools are saving you time, that time is almost certainly being spent seated. The lipid consequences are cumulative.
What does the latest clinical guidance say about cholesterol management for sedentary professionals?
The 2026 ACC/AHA Guideline on the Management of Dyslipidaemia - the most current international clinical standard, published in March 2026 - explicitly states that any physical activity is beneficial for sedentary individuals and should be encouraged to reduce cardiometabolic risk. It does not qualify this by exercise intensity. For desk-based South Asian professionals, the guideline’s framing reinforces what occupational health data has shown: reducing uninterrupted sitting is a first-line metabolic intervention, not a lifestyle suggestion. Combined with regular lipid screening, this is how early-stage dyslipidaemia is caught and reversed before it requires pharmacological management.
My recent blood work shows high triglycerides but normal LDL. Should I be concerned?
Yes. Elevated fasting triglycerides are not a minor finding - they are an independent cardiovascular risk factor and a direct marker of impaired LPL activity. High triglycerides with normal LDL often signals a pattern called atherogenic dyslipidaemia: elevated VLDL, small dense LDL particles (which are far more arterially damaging than large LDL particles), and suppressed HDL. A standard lipid panel may not capture small dense LDL. If your triglycerides are elevated and you have a sedentary desk job, ask your physician about an extended lipid subfraction analysis. 'Normal LDL' does not mean normal risk. It means the standard test did not look hard enough.
What are the early warning signs of high cholesterol I should watch for?
There are none. This is the clinical reality that makes dyslipidaemia uniquely dangerous: high LDL-C and elevated triglycerides produce no symptoms until a vascular event - a myocardial infarction or stroke - occurs. There is no pain, no fatigue specifically attributable to arterial plaque, no physical sensation as cholesterol deposits build up in the coronary endothelium. The chronic afternoon brain fog and lethargy you experience are metabolic signals worth investigating, but they are not cholesterol symptoms.
Final Words
Plaque does not announce itself. It accumulates quietly - inside the left anterior descending artery, around the coronary bifurcations, in the exact architecture of your heart’s blood supply - for years, sometimes decades, before it becomes an emergency. Then one morning, a plaque cap that has been thinning silently for years ruptures. A clot forms instantly. Blood supply to the myocardium ceases.
That rupture doesn't happen to unhealthy-looking people. It happens to the 38-year-old executive who passed his last physical, ran a 10K last month, and had absolutely no idea that his LDL particle count had been quietly destroying his coronary endothelium for the past four years.
There are no points for not knowing. Get screened. Now.
DISCLAIMER: This article is for preventative educational purposes only and does not constitute individual medical advice. If you are experiencing cardiac symptoms, please seek emergency medical care immediately.

Dr. Munazza
A General Physician (MBBS) with 5+ years of experience, currently working as an RMO at Saifee Hospital, focused on diagnosing, treating, and managing common health conditions.