
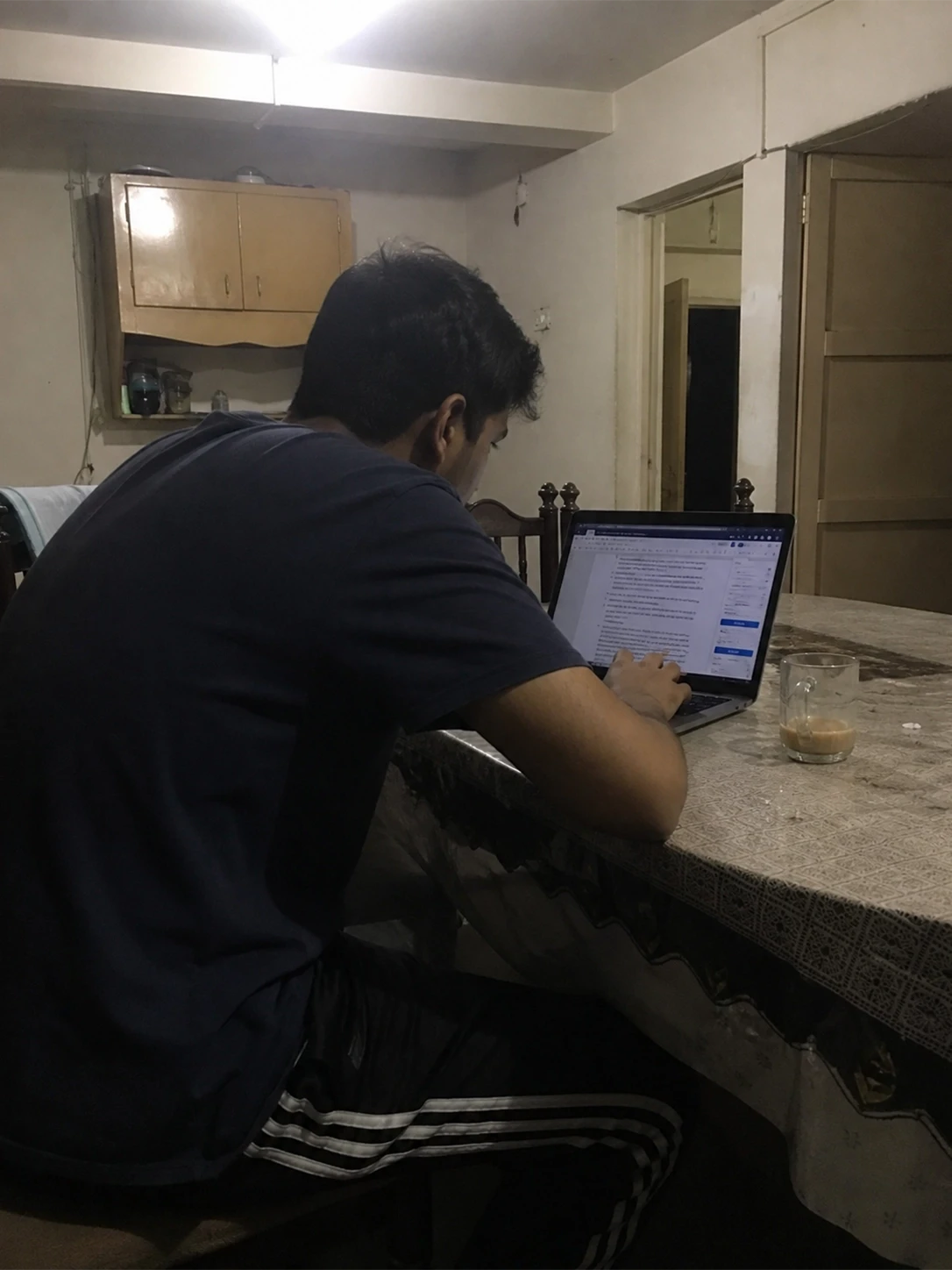
I did a home visit last week - a 27-year-old content manager in Gulshan-e-Iqbal, working remotely for a Dubai-based firm. She was hunched over a laptop balanced on a dining chair, dupatta draped over her shoulders, no proper desk in sight. The K-Electric schedule had her setup migrating between rooms all day - bedroom to lounge to kitchen counter, never once at the right height. Her neck was locked in 40 degrees of forward flexion for nine, ten, sometimes eleven hours at a stretch. When I placed my hand on her upper trapezius, I could feel the trigger points before I even pressed. Hard, dense, like marbles buried under the skin. She told me she thought the headaches were from the heat and stress of managing two kids while meeting deadlines. They were partly that. But mostly, they were coming from her cervical spine..
This is what I see across Karachi's remote-work population right now. AI tools - ChatGPT, Copilot, Gemini - have increased screen engagement hours dramatically while simultaneously removing the micro-movements that used to interrupt a workday: the walk to a colleague's desk, the physical retrieval of a document, the brief reprieve of a printer queue. A 2025 report from the International Labour Organization specifically flagged AI-managed, algorithmically driven workflows as deepening sedentary exposure in desk-based roles. The result is longer unbroken screen sessions, less postural variation, and a generation of professionals whose cervical spines are quietly deteriorating. Between 27% and 48% of office workers experience neck pain annually, according to a 2025 University of Miami clinical report - and those figures were recorded before AI productivity tools became as embedded in daily workflows as they are now.
The average person now spends nearly seven hours a day on screens, according to 2025 global data. For Karachi's tech professionals, that number is conservative. Add unreliable power infrastructure forcing emergency laptop sessions in awkward positions across multiple rooms, and you have a population absorbing enormous cervical spinal loads with no clinical support structure around them. No amount of Panadol, Volini spray, or phuphee's advice to 'sit up straight' is going to resolve a deep cervical flexor inhibition pattern. What follows is the clinical reality of what forward head posture actually does to your spine - and why the only way out involves rebuilding the muscles, not stretching them.
What Your Neck Is Telling You - and What It Actually Means
The Physical Symptom | The Biomechanical Reality | The Fatal Mistake |
Burning tension at the base of the skull | Suboccipital muscles - the four small muscles connecting the skull to C1/C2 - are in sustained isometric contraction, restricting blood flow and compressing the greater occipital nerve. This produces the classic 'vice grip' cervicogenic headache pattern. | Taking ibuprofen and returning to the same posture within the hour. |
Numbness or tingling running into the fingers | Forward head posture increases compressive load on the C5–C7 nerve roots - the segments supplying sensation and motor function to the arm. Tingling in the ring and little finger specifically suggests ulnar nerve involvement. This is not a circulation issue. It is a nerve impingement issue. | Shaking out the hands and assuming it will pass. It will - temporarily. Then progressively less so. |
Constant upper trapezius tightness | The upper traps are chronically overloaded because the deep cervical flexors - the muscles that should be stabilising the head - have effectively switched off. The trapezius compensates. It was not designed to do this for 9 hours. The trigger points you feel are ischaemic muscle knots formed from accumulated metabolic waste in chronically contracted fibres. | Aggressive massage or asking someone to 'crack' your neck. This temporarily relaxes the knot without addressing the underlying muscular imbalance. |
Jaw clenching and jaw pain (TMJ symptoms) | Forward head posture forces the mandible posteriorly, altering the resting occlusion and chronically loading the temporomandibular joint. The muscles of mastication - particularly the masseters - respond by clenching, especially during periods of screen concentration. This is not a dental problem. It begins in the neck. | Going to a dentist for a night guard without addressing the postural root cause. You will grind through the guard. |
The Biomechanics of Tech Neck
This is not about bad habits. It is about physics and what sustained, unloaded postures do to biological tissue over time. The clinical picture of tech neck is a chain reaction - one structural compromise setting off the next.
1. The 60-Pound Head: What Forward Head Posture Actually Costs Your Spine
In neutral alignment - ears directly over shoulders - your head weighs approximately 10 to 12 pounds. That is a manageable load for a healthy cervical spine. Now lean it forward three inches toward your monitor. The effective load your cervical musculature must support jumps to roughly 42 pounds. At four inches forward - which is common in laptop users working without a stand - that load reaches 60 pounds. A landmark study published in the European Spine Journal (2025) confirmed that a 60-degree forward tilt of the head - entirely typical of someone reading a phone on their lap - exerts up to 60 lbs of force on the cervical spine.
Your posterior neck muscles - the semispinalis, splenius capitis, and those small suboccipital muscles at the base of your skull - were not designed to hold 60 pounds of static load for eight hours. They fatigue within minutes. Once fatigued, they stop contracting and start accumulating metabolic waste: lactic acid, inflammatory cytokines, bradykinin. That tight, burning, wrapped-around-the-skull sensation you feel at 4 PM? That is tissue ischaemia. That is physiology. Not stress.
2. Upper Crossed Syndrome: The Muscular Imbalance Nobody Tells You About
Tech neck does not just affect your neck in isolation. It produces a predictable global muscular imbalance that physiotherapists call upper crossed syndrome. Here is the pattern: your pectoralis minor and upper trapezius become short and hypertonic - chronically tight. Your deep cervical flexors (longus colli, longus capitis) and lower/mid trapezius become long and inhibited - chronically weak. Your head migrates forward. Your shoulders round. Your thoracic spine flexes into a mild kyphosis.
A 2025 Frontiers in Pain Research study measuring posture-based classification of office workers found that habitual slumped sitting postures were directly associated with increased posterior pelvic rotation, thoracic flexion, and forward head posture - a full-chain kinetic collapse. The shoulder tension you feel is a symptom of this imbalance, not the cause. No amount of shoulder rolling or heat packs will correct an upper-lower muscle imbalance. You have to reload the deep stabilisers.
3. The Suboccipital Spasm: Why Your Headaches Start in Your Neck
Stop me if this sounds familiar. You are three hours into a Teams call. Your chin has gradually climbed upward - partly because your screen is slightly too low, partly because your thoracic spine has rounded so far that looking straight requires tilting your face toward the ceiling. Your suboccipital muscles - rectus capitis posterior major and minor, obliquus capitis - are in sustained contraction.
These four small muscles connecting the base of your skull to C1 and C2 do not just move your head. They contain a disproportionately high density of muscle spindles - proprioceptive receptors that communicate with your cerebellum and contribute to gaze stabilisation. When they are chronically contracted, they compress the greater occipital nerve (GON) as it passes through them. The result is cervicogenic headache: pain that starts at the base of the skull, radiates over the scalp to the forehead, sits behind one or both eyes, and is frequently misidentified as a tension or migraine headache. Unlike a true tension headache, cervicogenic headache is reliably reproduced by sustained neck postures. If rotating your neck in a certain direction reliably brings on your headache, you are not dehydrated. Your neck is referring pain.
4. The Ergonomic Illusion: Why Your Rs.80,000 Chair Isn't Fixing Anything
I have walked into home offices with standing desks, lumbar supports, monitor arms, and wrist rests - all purchased and positioned thoughtfully - where the person still has tech neck, cervicogenic headaches, and bilateral shoulder tightness. Equipment cannot compensate for muscular deficiency.
Your cervical stabilisers - specifically the deep cervical flexors (longus colli and longus capitis) - are the active restraint system of your neck. When they are inhibited or weak, no passive support substitutes for them. Research published in PubMed (Systematic Review, Clinical Rehabilitation) found strong evidence that deep cervical flexor training specifically addresses the neuromuscular coordination deficit in chronic neck pain - not because it builds bulk, but because it retrains the inhibited firing patterns of these muscles. An ergonomic chair does nothing for inhibited firing patterns.
Similarly, a 2025 meta-analysis published through Physical Therapy (Oxford Academic) found moderate-quality evidence that neck and shoulder strengthening exercises - not ergonomic interventions alone - produced the largest effect sizes for reducing neck pain in symptomatic office workers. The chair is a variable. The muscle is the mechanism.
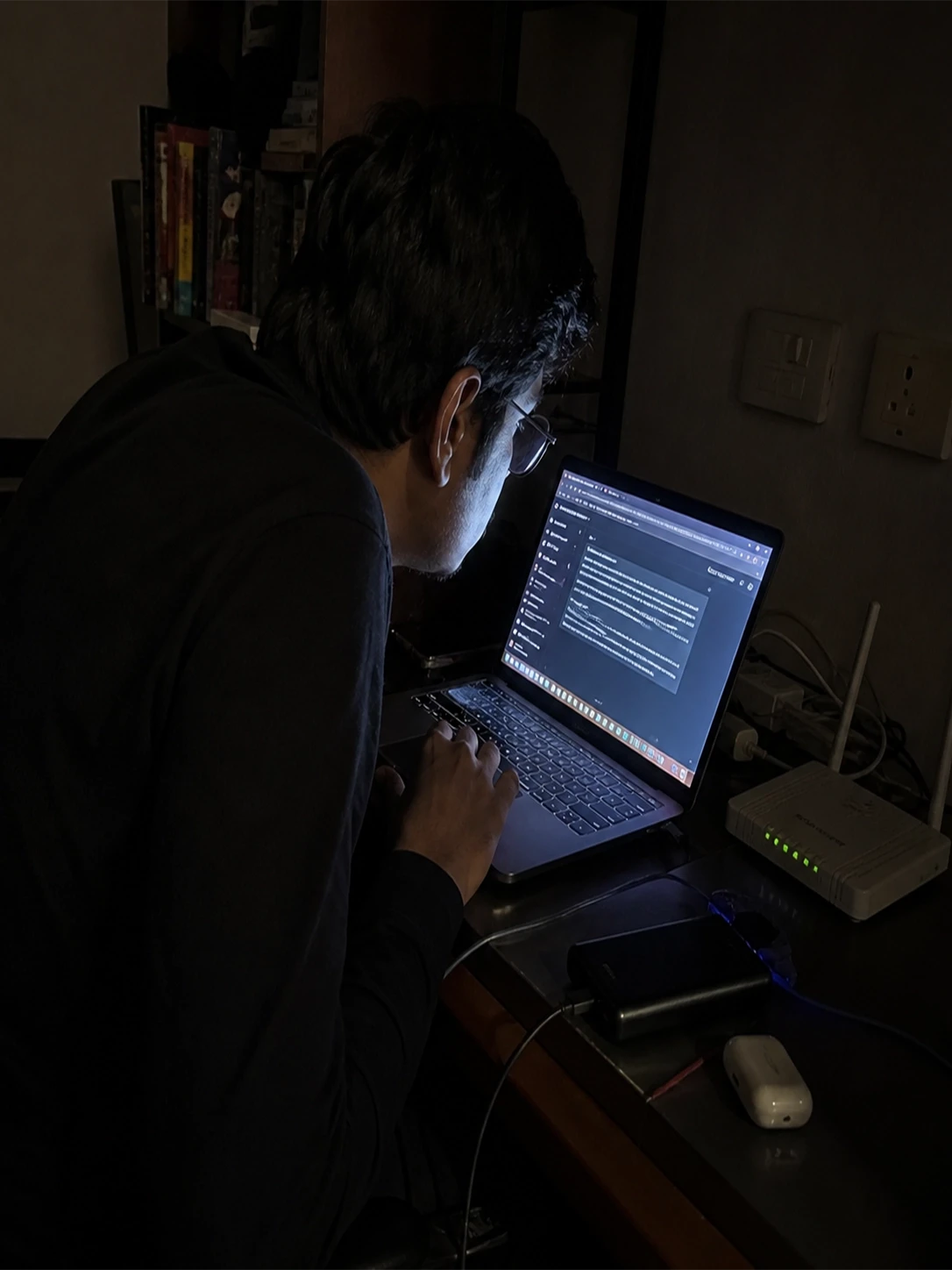
5. The AI Workday: More Productive, More Static, More Damaged
Here is what the ergonomics literature has not fully caught up with yet. AI productivity tools are not just changing what we do at our desks - they are changing how long we sit without moving while doing it. Before ChatGPT and Copilot became embedded in daily workflows, a knowledge worker's day contained dozens of natural postural interruptions: walking to a printer, standing to brief a colleague, moving between rooms, waiting for a document to load. These were not inefficiencies. They were involuntary movement breaks - micro-interruptions of cervical loading that gave the suboccipital muscles and deep cervical flexors time to recover.
AI tools have compressed those interruptions out of the day. Tasks that required physical movement now resolve in a single prompt. The ILO's 2025 occupational health report explicitly identified AI-managed, algorithmically driven work as deepening sedentary exposure and increasing ergonomic risk in desk-based roles - particularly the risk of prolonged static cervical loading. A 2025 study in the Journal of Occupational and Environmental Medicine found that remote workers logging longer screen hours with poorer workstation setups had double the odds (OR = 2.02) of developing new neck or upper back pain compared to office-based workers - a risk directly proportional to uninterrupted screen time.
If your AI tools are saving you two hours of task time per day, those two hours are almost certainly being spent at the same screen, in the same posture, compounding the cervical load rather than relieving it. Efficiency without movement is not productivity. It is a slow structural injury.
The Fatal Desk-Posture Mistakes Karachi's Professionals Keep Making
Reaching for muscle relaxants (Flexon, Myoril) instead of addressing the biomechanical root cause. Muscle relaxants reduce the protective guarding of already-hypermobile cervical segments. You feel looser. You are actually less stable. The pain returns - usually worse.
Aggressive static neck stretching without first strengthening the opposing muscles. Stretching a chronically overstretched muscle - which is exactly what the posterior neck muscles are - increases laxity in already-compromised capsular ligaments. Stop pulling your ear to your shoulder and start loading your deep cervical flexors.
Positioning the primary monitor off to one side. This forces sustained cervical rotation - a sustained rotational load on already-compressed facet joints and unilateral scalene tightness. Your primary screen must be directly in front of you. Non-negotiable.
Working on a laptop in bed or on a sofa. The flexion angle of the cervical spine in these positions is clinically indefensible. Every minute you spend hunched over a laptop on your mattress is a minute spent compressing cervical discs under asymmetric load.
Asking your sibling to walk on your back or aggressively cracking your neck. You are destabilising hypermobile segments while completely ignoring the weak, inhibited muscles causing the actual tension. A hypermobile joint that keeps 'needing' to be cracked is a joint that has lost its active muscular restraint. That is a clinical problem, not a massage problem.
Relying entirely on AI-generated posture tips without clinical assessment. The AI does not know whether your headaches are cervicogenic or vascular in origin, whether you have early disc disease at C5/C6, or whether your thoracic restriction is driving your forward head posture. These distinctions require a physical examination.
Rapid-Fire Clinical FAQs
Why do I get severe headaches behind my eyes after working on my laptop?
These are almost certainly cervicogenic headaches - pain generated by the cervical spine and referred to the orbital region via the trigeminal-cervical complex. The suboccipital muscles (rectus capitis, obliquus capitis) compressing the greater occipital nerve produce exactly this pattern: base-of-skull origin, radiation over the scalp, pressure behind one or both eyes. If the headache is reproduced or worsened by specific neck positions, it is not a migraine - it is your neck.
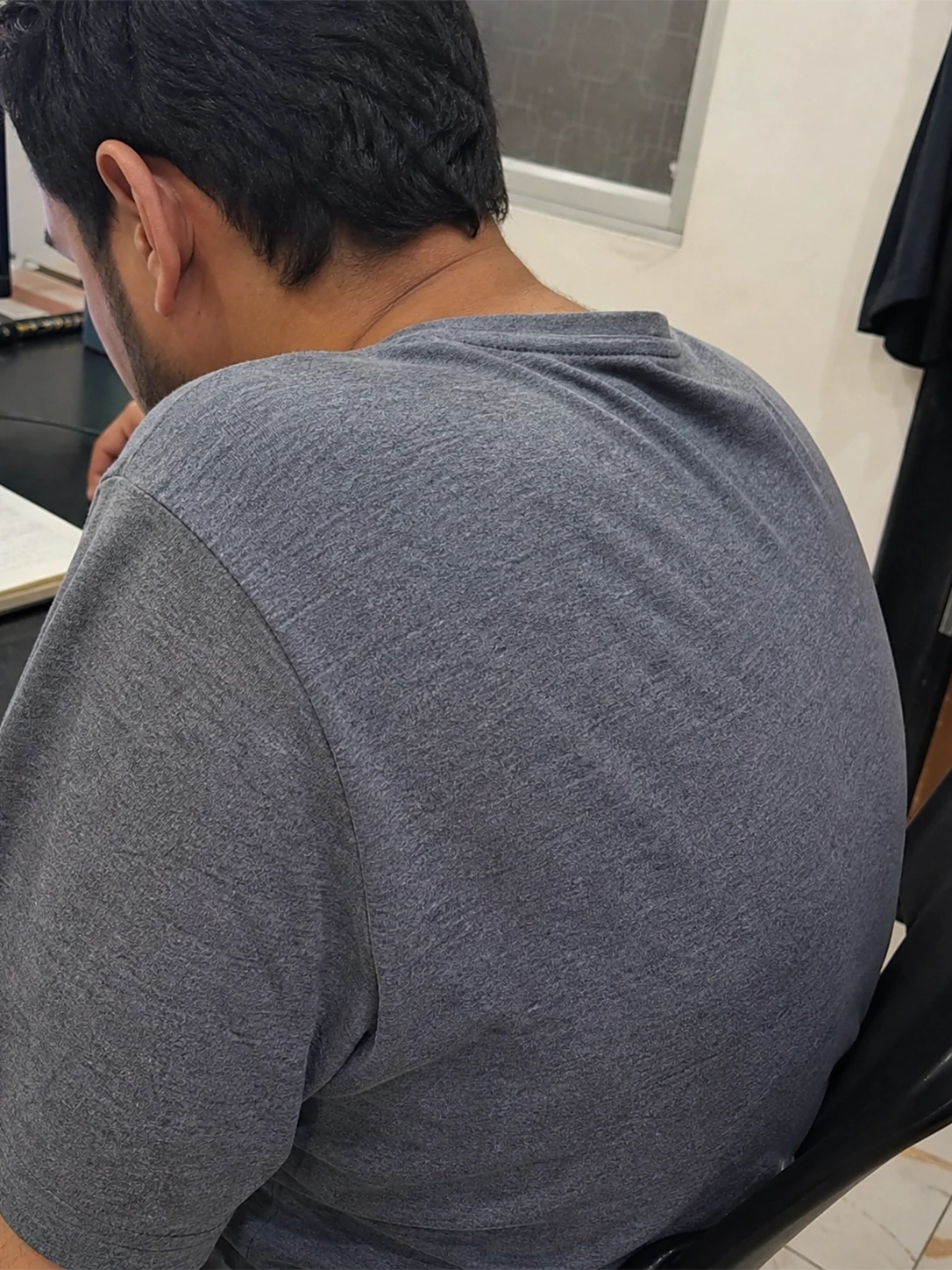
How can I fix the 'hump' forming at the base of my neck?
What you are feeling is a combination of C7/T1 prominence and superficial fat pad accumulation - a direct consequence of sustained thoracic flexion and forward head posture. The bone itself is not changing; the soft tissue around a chronically loaded segment hypertrophies. Correcting it requires thoracic extension mobility work, deep cervical flexor strengthening to pull the head back over the shoulders, and scapular retractor loading (mid/lower trapezius, rhomboids) to open the chest. Postural taping can provide proprioceptive cueing during rehabilitation. This does not happen overnight - expect 8 to 12 weeks of consistent targeted rehab with a physiotherapist guiding load progression.
Is it normal for my hands to feel tingly when my neck is stiff?
No. This is a red flag that requires urgent clinical assessment. Tingling in the hands in association with neck stiffness suggests cervical radiculopathy - compression or irritation of a nerve root in the cervical spine, most commonly C6 or C7. Tingling in the thumb and index finger points to C6; tingling in the middle finger suggests C7; ring and little finger suggest C8 or ulnar nerve involvement. None of these should be self-managed with stretching or massage. If you are experiencing progressive numbness, hand weakness, or symptoms that wake you from sleep, seek clinical evaluation immediately.
What are the best 2-minute desk exercises to relieve trapezius pain?
The most clinically effective immediate intervention is the chin tuck (cervical retraction): sitting upright, gently draw your chin straight back - not down - until you feel a mild stretch at the base of your skull. Hold for 3 seconds, release, repeat 10 times. This directly activates the deep cervical flexors and mechanically deloads the upper trapezius. Pair it with scapular retraction: shoulders back and down, squeezing the mid-trapezius and rhomboids for 5 seconds. These two exercises address the actual biomechanical dysfunction - inhibited stabilisers - not just the symptom.
Can poor neck posture actually cause jaw pain and TMJ issues?
Yes - and this is a consistently underdiagnosed connection. Forward head posture posteriorly displaces the mandible, altering the resting position of the condyle within the temporomandibular joint. The masseters and pterygoids compensate by clenching to maintain resting occlusion, creating chronic compressive load on the TMJ disc. Research on the cervical-mandibular relationship confirms that FHP significantly alters mandibular position and muscle activation patterns. If you are waking up with jaw soreness or jaw fatigue during screen sessions, your neck is very likely implicated. Treatment addressing the cervical dysfunction - not just dental splints - is clinically indicated.
Does wearing a posture-corrector brace actually work for tech neck?
Short answer: not in any way that matters long-term. A posture brace passively holds your shoulders back without engaging the muscles responsible for maintaining that position. You are outsourcing the work to a piece of elastic rather than rebuilding the neuromuscular control that is the actual problem. Prolonged brace use can actually further inhibit the already-weak scapular retractors and deep cervical flexors by reducing the demand on them. Use a brace for no more than 2 hours as a proprioceptive reminder during early rehab, not as a treatment. The goal is active muscular endurance, not passive restraint.
How often should I take screen breaks to protect my cervical spine?
The evidence-based recommendation is a postural break every 30 to 45 minutes of sustained screen use - not the 2-hour intervals most people actually take. Each break should include a chin tuck series, a brief standing period, and cervical range-of-motion rotation (not stretching - active movement). If you are using AI productivity tools that extend unbroken screen sessions, set a dedicated movement timer.
Final Words
The cervical spine has seven vertebrae, 23 intervertebral disc surfaces, and an intricate network of nerve roots supplying every structure below the neck. It was engineered for dynamic movement - rotation, flexion, extension, lateral tilt - not sustained isometric loading under 42 to 60 pounds of compressive force. Every hour spent in uncorrected forward head posture is an hour of disc compression, facet loading, and deep stabiliser inhibition that accumulates structurally.
Disc degeneration at C5/C6 and C6/C7 - the segments most heavily loaded in sustained FHP - does not declare itself until it is advanced. The first symptom is sometimes not neck pain at all. It is a numb hand, a weakened grip, or a referred pain that the patient has been treating as a shoulder problem for two years.
The screen is not going anywhere. The AI workload is not shrinking. But the structure of your cervical spine is finite, and it is already absorbing the cost of your efficiency.
Sehat Door At-Home Physiotherapy & Posture Assessment - Book Now

Dr. Aleena PT
A Physiotherapy Doctor (DPT) from Jinnah Sindh Medical University, focused on musculoskeletal rehabilitation, evidence-based patient care, pain management, mobility improvement, and recovery support.