
It starts quietly. By 8 pm you've finished work, closed the laptop, and stepped outside into Karachi's night heat - that specific, wet, 34°C kind that doesn't feel like evening at all. The commute on Shahrah-e-Faisal is forty-five minutes of horns and diesel fumes. You reach home to find there's been load-shedding since seven. The room is hot, the UPS has died, and your mother is on the phone asking when the school fees are due. You eat whatever is on the stove standing up, skip water entirely, and lie down.
It comes at some time around midnight. Not a headache. Something else. A pulsing behind one eye, deep and rhythmic, as if something were pushing outward behind the skull with every heartbeat. Light from the small emergency lamp makes it worse. The generator starts across the street and the sound is unbearable. Nausea sits at the back of your throat. You have a presentation tomorrow.
You take a painkiller and spend the next six hours waiting for morning.
If this is your life, you are not weak, you don't need to imagine it, and you are not 'just stressed.' You suffer from migraine - a genuine neurological disease that affects roughly one in seven people worldwide. According to a 30-year global burden analysis published in Pain and Therapy (2025), the worldwide number of people living with migraine has grown by over 58% since 1990, now reaching 1.16 billion cases. It remains one of the top causes of disability-adjusted life years globally, with a disproportionate burden on women aged 30 to 44. The unique mix of heat, air pollution, financial pressure, erratic sleep schedules, and excessive screen time in Karachi doesn't create migraine from nothing - it simply makes a migraine-prone brain fire far more often than it should.
This guide is not about perfecting your lifestyle. It's about understanding why your migraines keep coming back, and making the smallest realistic changes that can actually lower how often they happen.
Why Migraines Keep Coming Back: The Trigger Cluster Table
Before anything else, understand this: your migraines are not random. They follow patterns tied to your specific life. The table below maps common Karachi situations to what is actually happening in the migraine brain, and gives you one thing you can do about each.
Karachi Life Situation | What It Does to a Migraine Brain | One Preventive Move You Can Actually Make |
Working 9+ hours on screens, skipping lunch, drinking chai instead of water, then commuting home in 35°C heat | Dehydration, low blood sugar, eye strain, and accumulated stress lower your migraine threshold - making an attack much more likely. | Carry a 1-litre water bottle and finish it during work. Cap chai at your usual amount. Never skip meals - even biscuits count. |
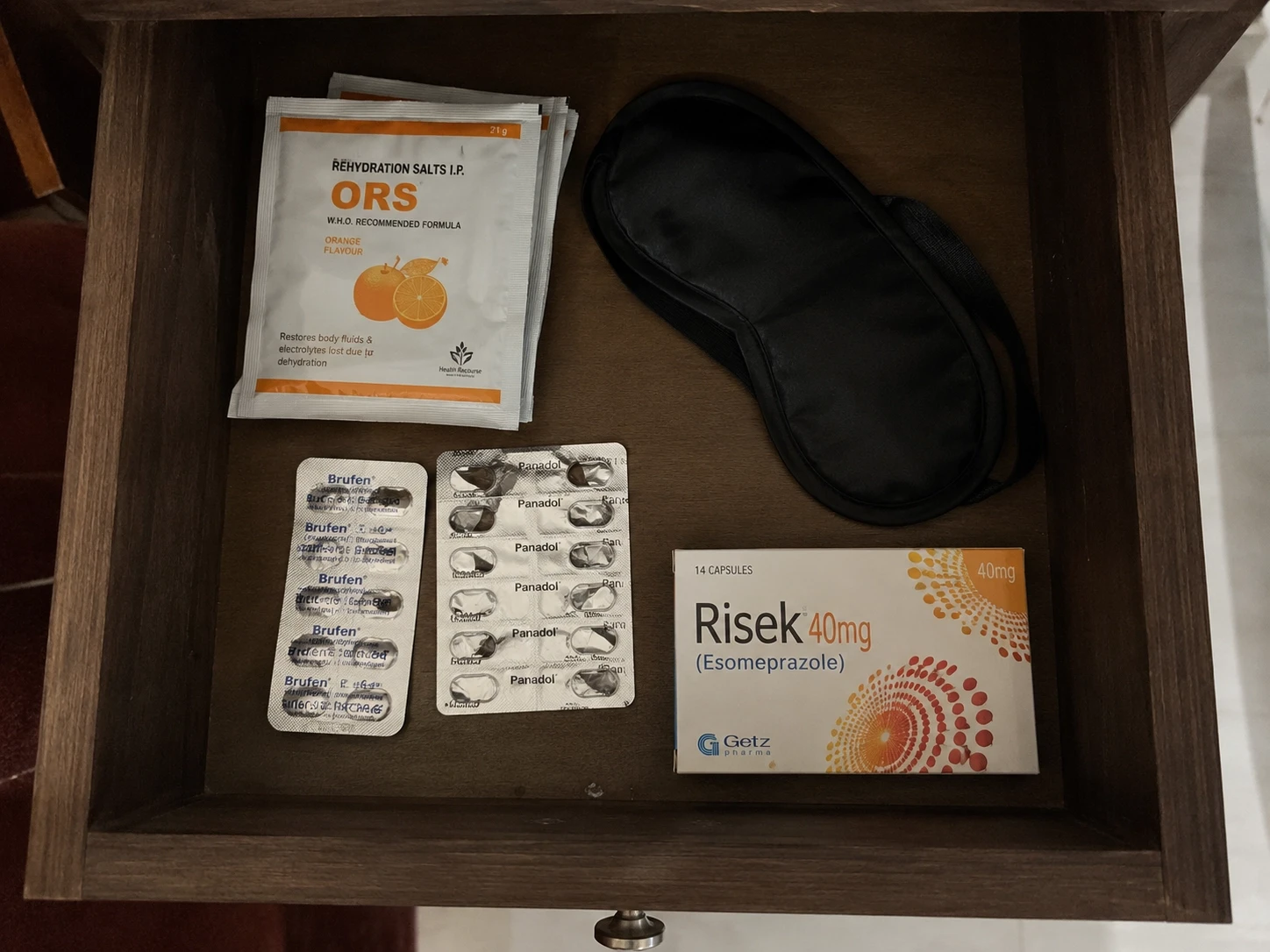
Reaching home to load-shedding: no fan, no AC, cooking in heat, noise and family stress about bills or rent | Heat, sensory overload, and stress hormones spike together - a well-known combination for triggering attacks. | Keep a 'migraine corner' ready: cold pack or wet cloth, water, light snack, and medications in one drawer so you can step away before the attack peaks. |
Sleeping at random times because of work overload and power cuts - three or four different sleep times in a single week | Irregular sleep is one of the strongest lifestyle triggers. It disrupts the brain rhythms migraine is acutely sensitive to. | Aim for roughly similar sleep and wake times, even on weekends. If you sleep late, keep the shift smaller instead of swinging by three or four hours. |
Constant worry about rent, school fees, or job loss, layered on top of household and caregiving responsibilities | Chronic stress doesn't directly 'cause' migraine but keeps the brain on high alert, making every other trigger hit harder. | Use short daily stress valves: 5–10 minutes of quiet breathing, a brief walk, or sitting in a dark room with no phone. Seek medical help if anxiety symptoms are significant. |
How Migraine Happens and Why Triggers Matter
Migraine Brain 101: Your Head Is Not 'Too Weak'
On the nights before exam-season corrections, my aunt - a schoolteacher in Gulshan-e-Iqbal, two kids, husband working long shifts - used to go to bed at 4:00 AM. She'd wake at 6:30 AM feeling as if the top of her skull had been pressed in a vice. For years, her family told her it was 'weak eyesight' or 'tension.' Her colleagues suggested she just needed a vacation.
In reality, something entirely different was happening. Migraine is a genetic neurological condition. The brain of someone with migraine is not weak - it is, neurologically speaking, hyperexcitable. The trigeminal nerve, one of the largest nerve pathways in the skull, is more easily activated. Certain inputs - a temperature change, a hormonal shift, a skipped meal, one particularly brutal commute - trigger a cascade of electrical activity called cortical spreading depression, a wave of suppressed brain activity that rolls across the cortex and activates pain pathways. The brain releases a peptide called CGRP (calcitonin gene-related peptide), which dilates blood vessels, fires pain signals, and causes that deep, pulsing, one-sided headache you know too well. The surrounding scalp becomes so sensitive that even a pillow touching your head hurts. That sensitivity is called central sensitization.
A typical migraine moves through phases. The prodrome can start one to two days earlier - subtle changes like food cravings, neck stiffness, irritability, or unusual yawning that most people never connect to the attack coming. Some people experience an aura: temporary visual disturbances (zigzag lines, blind spots), tingling on one side of the face or hand, or briefly slurred speech. The headache phase follows - moderate to severe, throbbing, typically one-sided, worsened by movement, light, and sound. The postdrome lingers after the pain fades: exhaustion, the 'head feels bruised from inside' feeling, difficulty thinking clearly.
Triggers do not cause migraine. They lower the migraine threshold - the point at which this sensitive brain tips into an attack. Understand that distinction, and you stop blaming yourself for every attack, and start managing your threshold instead.
Heat, Dehydration, and Karachi's Summer as a Migraine Trigger
From June to September in Karachi, it is no exaggeration to say that it is one of the most challenging environments on earth for someone with migraine. Temperatures push past 38°C, humidity sits near 80%, the glare off the road at 3 pm is blinding, and load-shedding guarantees that a significant part of the day will be spent without cooling.
The connection between heat and migraine is real and increasingly documented. A 2025 scoping review in Brain and Behavior found individual-level associations between ambient temperature and migraine attacks, with 83% of patients in one study reporting weather as a trigger. Research found that for every 10°F increase in outdoor temperature, headache occurrence rose by 6%. A September 2025 cohort study found that individuals who experienced heat-related illness were more than twice as likely to develop chronic migraine in the five years that followed, compared to matched controls.
The mechanism is straightforward. Heat drives sweating and fluid loss, shifting your electrolyte balance. The body works harder to maintain temperature, triggering stress hormones and vascular changes. Bright sunlight and glare activate the trigeminal nerve directly. Put heat + dehydration + a missed meal + a loud commute together and you have stacked four separate threshold-lowering triggers into a single evening.
What you can actually do in Karachi:
Drink one glass of water every time you open your phone after a meeting. Most office workers in Karachi are mildly dehydrated by 3 pm without noticing.
Keep a sachet of ORS in your bag in June. Not because you are ill - because your electrolyte balance matters on a 38°C day.
If you are commuting in the afternoon heat, try a damp cloth on the back of the neck. It lowers perceived body temperature faster than a cold drink.
Carry sunglasses with FL-41 tinted lenses if strong light is a consistent trigger. The amber-rose tint is specifically effective for light-triggered headache.
On load-shedding evenings, prioritise the 'migraine corner' - wet cloth, dark space, water - before an attack fully escalates. The window to abort or reduce it is narrow.
Stress, Overwork, and the 'Tired But Wired' Brain
There's a specific feeling Karachi's working population knows well. It's not tiredness exactly. It's the state of being simultaneously exhausted and unable to switch off - lying in the dark with the ceiling fan overhead, replaying the argument about electricity bills, mentally calculating whether the bonus covers the school fee instalment, refreshing email at 11:30 pm. The brain is depleted. But it won't quiet down.
Stress is consistently the most reported migraine trigger, and the relationship runs in both directions: stress raises attack frequency, and recurring attacks increase anxiety about when the next one is coming - a cycle that can gradually transform episodic migraine into chronic migraine (15 or more headache days per month). A 2024 cohort study in Cephalalgia found that higher migraine headache intensity was directly associated with higher occupational burnout scores, with workers losing a median of three days per month to reduced productivity - independent of absenteeism. For the call centre employee in Clifton, the teacher managing forty students before noon, or the homemaker absorbing domestic friction while managing load-shedding and grocery inflation: that data describes a real, documented process happening in your brain.
Realistic stress management for a Karachi workday:
Three-minute breathing between tasks: slow exhale, not dramatic 'cleansing' breaths. The goal is to drop sympathetic nervous system activation, not perform wellness.
A no-phone window of 20–30 minutes after finishing work, before eating dinner. Notifications are small cortisol spikes. The brain needs the gap.
Walking - even just to the corner shop and back - counts as a movement snack that reduces migraine frequency with no equipment required.
If you notice anxiety, low mood, or persistent dread alongside your migraines, that is medically relevant. Untreated anxiety and depression are known risk factors for migraine chronification. Raising this with a doctor directly affects your migraine outcome.
For a deeper look at how chronic screen exposure and cognitive overload affect sleep and stress in exactly this population, SehatDoor’s guide on screen-time insomnia is worth reading alongside this one.
Sleep, Meals, and Caffeine: The Everyday Triggers You Keep Underestimating
I've had patients tell me their migraines 'come from nowhere.' Then I ask about their sleep that week. It turns out they went to bed at midnight Monday, 3 AM Tuesday, fell asleep on the sofa at 9 PM Wednesday, were up at 6 AM Thursday for a meeting, and slept till noon on Friday. That is not 'normal variation.' That is the kind of rhythmic disruption that a migraine brain cannot handle.
A 2025 cross-sectional study on lifestyle factors in chronic migraine found that poor sleep quality, high stress, and excessive caffeine intake were the three factors most significantly associated with increased migraine frequency. Regular physical activity and consistent meal patterns were inversely related to monthly migraine days.
Sleep
You don't need a perfect 8 hours. You need consistency. If you typically sleep at 11:30 PM and wake at 6:30 AM, hold that pattern on weekends too. An hour of drift is acceptable. Three hours is a trigger. Load-shedding disrupts this badly. A small pedestal fan on a timer, earplugs for the generator noise, and switching your phone to grayscale after 10 PM are unglamorous but effective. Detailed practical guidance on how blue light and late screens damage sleep quality is available separately on SehatDoor.
Meals
Skipping breakfast and lunching at 3 PM is migraine kindling. Blood sugar drops activate stress hormones, which lower your threshold. The American Migraine Foundation recommends smaller, regular meals - ideally six modest meals across the day - to stabilise blood sugar. In a chaotic work schedule, this means keeping almonds, a banana, or a small box of biscuits in your bag so you are never more than three hours without something in your stomach.
Caffeine
This one is counterintuitive and important. Caffeine can abort a mild migraine attack because it constricts blood vessels and amplifies analgesics. But caffeine consumed inconsistently - three cups today, one tomorrow, none the day after - creates withdrawal headaches indistinguishable from migraine. The Cleveland Clinic’s SEEDS framework for migraine management recommends a stable, low daily intake - ideally under 200 mg - rather than quitting abruptly or spiking on high-stress days. For most Karachi chai drinkers: two cups, at roughly the same time each day, no sudden changes. If you are currently at five cups, reduce by half a cup every two weeks. Abrupt withdrawal will give you a five-day headache that has nothing to do with migraine triggers.
A 2025 narrative review on diet and migraine prevention confirms that irregular caffeine is among the most consistently reported dietary triggers, while Mediterranean-style eating - which overlaps significantly with the traditional Pakistani dal, sabzi, and chapati diet - shows promising protective effects. You may not need to change what you eat as much as you need to change when and how consistently you eat it.
From 'Random Attacks' to Pattern Recognition: The Power of a Migraine Diary
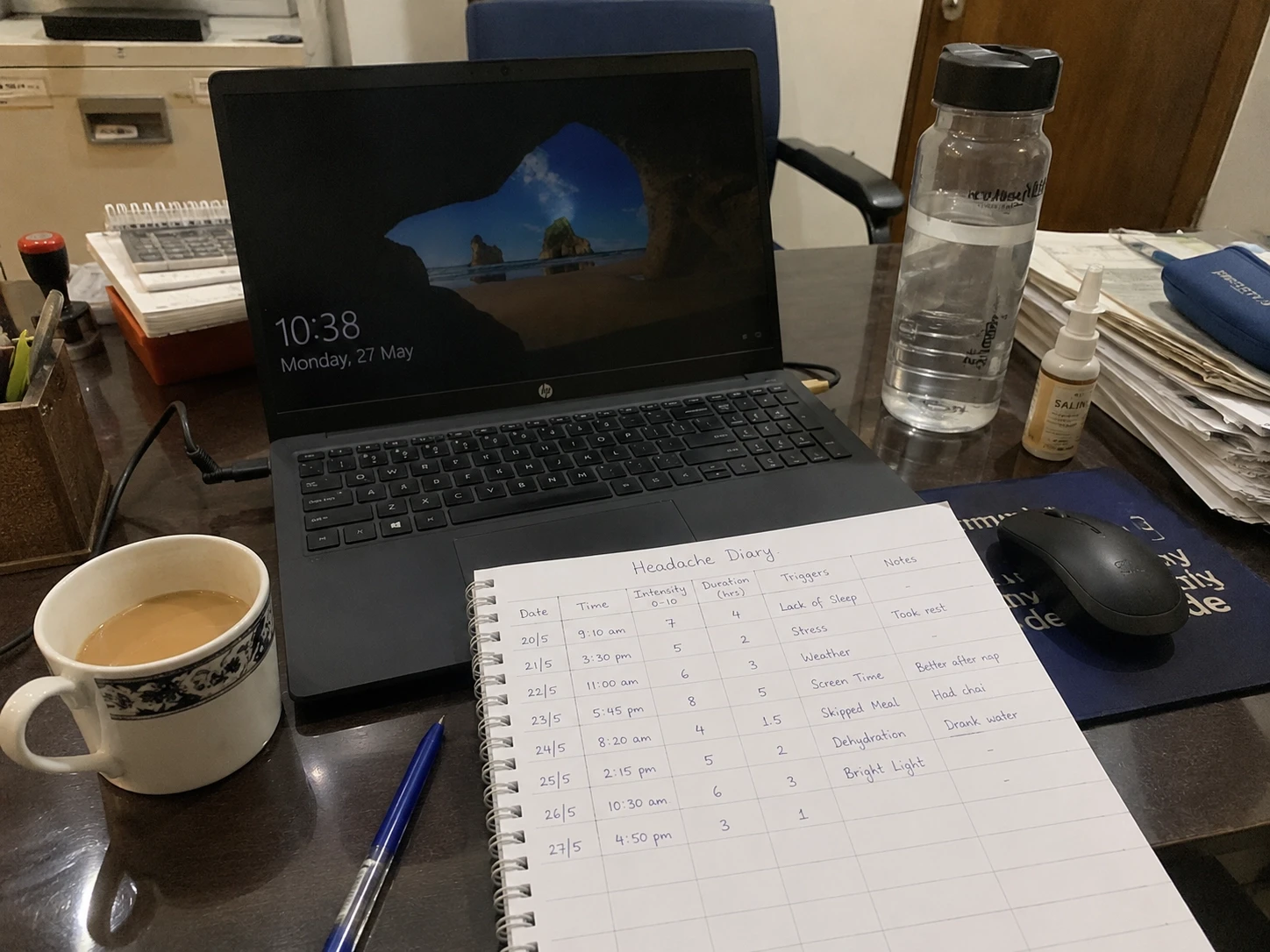
The single most useful clinical tool for migraine management costs nothing and requires about three minutes per day. It is a diary.
Not a complicated one. A note on your phone - or a small notebook - where after each headache you write down six things: the date and time it started, what you ate in the previous 12 hours, how you slept the night before, your stress level (1–10 is fine), whether the weather changed, and for women, where you are in your menstrual cycle. Within 6–8 weeks, most patients can see their own trigger clusters clearly. Not 'I have migraines.' But 'I have migraines on the second day after a late work night, when I skipped lunch and it was hot.'
That specificity changes everything. It tells you which triggers are fixed (hormones, weather) and which are modifiable (sleep, hydration, meals). It also gives your doctor something to work with - especially when deciding whether preventive migraine medications are appropriate.
Simple template: date | pain level (1–10) | side of head | food/drink past 12h | sleep last night | stress level | any other notes. Photograph it on your phone. That is your migraine diary.
Realistic Lifestyle Changes for Karachi: The SEEDS Framework, Adapted
The SEEDS framework - Sleep, Exercise, Eat, Diary, Stress - is used by migraine neurologists internationally as a structured approach to lifestyle management. Below is an honest, Karachi-specific version.
Sleep
The goal is consistency, not duration. Sleep and wake at approximately the same time daily. On load-shedding nights: use a battery-operated or rechargeable small fan if possible; keep earplugs near the bed for when the generator starts at 2 AM; avoid looking at your phone once you've lain down - the blue light suppresses melatonin and makes it harder to fall back asleep when power returns. Poor sleep in migraine is not just a lifestyle issue - it is a direct neurological trigger.
Exercise
Research supports 15–20 minutes of daily movement as beneficial for reducing migraine frequency - and you do not need a gym. Three 10–15 minute walks - morning, lunch break, and evening - count. The mechanism is real: regular moderate aerobic activity lowers CGRP levels and reduces central sensitization over time. Movement snacks are legitimate medicine for migraine prevention.
Eat
Regular meals, adequate water, stable caffeine. Small, protein-anchored meals beat large, irregular ones. In June and July: at least 2.5–3 litres of water daily, with electrolyte replacement if you are sweating heavily. ORS is inexpensive and underused as a migraine prevention tool in Pakistani summers.
Diary
Keep it simple. Use your phone. Six data points per attack. Bring it to every doctor visit. If you use a home doctor consultation in Karachi through Sehat Door your doctor can review the diary during the visit and help you identify your specific trigger cluster - far more useful than trying to reconstruct three months of attacks from memory in a ten-minute appointment.
Stress
Micro-interventions work when large ones are impractical. Three minutes of slow breathing between tasks. A 15-minute no-phone window before sleep. One weekly activity - even a brief evening walk in relative quiet - that is yours alone. If anxiety or depression is present alongside migraine, addressing both together produces better outcomes than treating migraine alone.
Rapid-Fire Clinical FAQs
1. How do I know if my headache is migraine or just stress and eye strain?
Migraine typically produces moderate to severe, throbbing, one-sided pain, worsened by movement, light, and sound, often with nausea. Stress headaches are usually bilateral, pressing rather than throbbing, and don't worsen with light or movement. Eye strain headaches ease with rest. If you're unsure, or if headaches are frequent, book a consultation - distinguishing between headache types matters because treatment differs.
2. Can Karachi's heat and load-shedding really trigger my migraines?
Yes. Heat, humidity, sudden temperature changes, and sensory overload from noise are documented migraine triggers. Load-shedding combines several at once. The 2025 research on ambient temperature and migraine specifically supports individual-level heat sensitivity as a real physiological phenomenon. Managing the environment - cooling, hydration, avoiding peak heat windows - is legitimate migraine prevention.
3. I work 9 hours on screens. What are the minimum changes I need?
Three non-negotiables: drink water consistently through the day (not just during headaches); do not skip meals, especially lunch; and take a 3–5 minute eyes-off-screen break every 90 minutes. If you wear glasses, get your prescription checked - uncorrected refractive error is a frequently overlooked contributor to eye-strain headaches that lower the migraine threshold.
4. When should I think about preventive migraine medicines?
Preventive medication is typically indicated when you have four or more migraine days per month, when attacks are severely disabling, when acute medications don't work well, or when you are taking acute treatment more than two days per week. This is a decision to make with a doctor - home doctor consultations in Karachi through Sehat Door make this accessible without a hospital visit.
5. Is it safe to take painkillers or triptans every time I get a migraine? How much is 'too much'?
Using simple analgesics on 15 or more days per month, or triptans on 10 or more days per month, causes medication overuse headache (MOH) - a condition where the medicine meant to treat your headaches is now causing them. The Migraine Trust calls this 'rebound headache', and it is one of the most common reasons episodic migraine becomes chronic daily headache. If you are taking any headache medication more than twice a week regularly, you need a medical review.
6. Can strong emotions, money stress, and family arguments actually trigger migraine attacks?
Yes - directly. Acute emotional stress causes a rapid surge in cortisol and adrenaline, activates the trigeminal pathway, and can push a sensitised brain into an attack within hours. The 'let-down migraine' - an attack that arrives on Friday evening after a high-stress work week ends - is a textbook example of this physiology. You are not imagining that a bad phone call gives you a headache.
7. When should I go to ER instead of lying in a dark room?
Go immediately if your headache is: the worst of your life and sudden ('thunderclap' onset); accompanied by fever, stiff neck, or rash; associated with confusion, slurred speech, vision loss, or arm/face weakness; or follows a head injury. These are red-flag symptoms requiring emergency evaluation to rule out meningitis, subarachnoid haemorrhage, or stroke. A typical migraine attack - even a severe one that fits your usual pattern - is not an emergency. But when something feels different, trust that instinct and get assessed.
A Final Word on Getting This Right
Migraine treated as 'just a headache' costs you. It costs you work days, missed dinners with your kids, relationships strained by cancelled plans, the anxiety of never knowing when the next attack is coming. It costs the quiet, grinding exhaustion of living around a condition you have never been given proper tools to manage.
The biology is clear: you have a sensitive neurological system that overreacts to a predictable set of inputs. Many of those inputs - sleep, hydration, meal timing, caffeine consistency, stress load - are partially within your control, even in Karachi's specific, unforgiving environment. Some are not. Heat is not going away. Financial pressure is not going away. Load-shedding is certainly not going away.
But the difference between someone who has six migraines a month and someone who has two is often not luck or willpower. It is pattern recognition, small consistent habits, and the right medical support when lifestyle management alone is not enough.
A home doctor consultation means you don't have to sit in a hospital waiting room with a migraine attack already underway. A physician can review your diary, assess whether preventive treatment is appropriate, check whether something other than migraine is contributing - including an at-home blood test to rule out deficiencies and other causes of chronic fatigue and headache - and help you build a plan that accounts for your specific life, not a generic patient profile.
Migraine that goes unmanaged for ten years does real damage - to your quality of life, your relationships, and your career. Getting it properly assessed now is not an indulgence. It is the cheaper, kinder choice in the long run.
Disclaimer: This article is general health education and does not constitute personalised medical advice. For diagnosis or treatment, consult a qualified physician.

Dr. Munazza
A General Physician (MBBS) with 5+ years of experience, currently working as an RMO at Saifee Hospital, focused on diagnosing, treating, and managing common health conditions.