
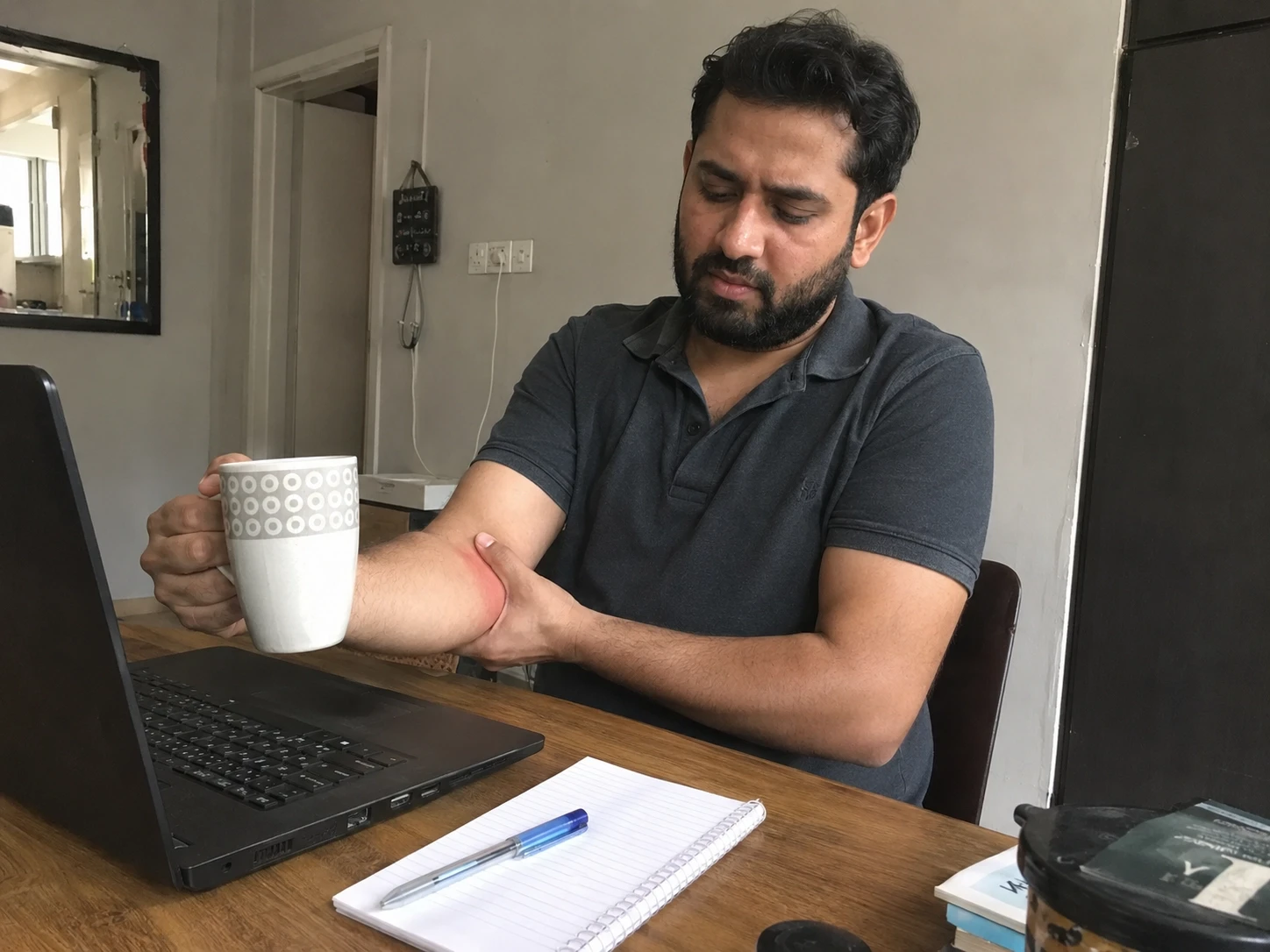
You've been feeling your elbow for a while now. Perhaps it began with a minor pain and pinch while picking up your cup of chai in the morning. Next it was there when you were gripping the car door, twisting a bottle open, or reaching for the mouse. Now it’s there every time you load grocery bags off the bike, pick up your child, or shake someone’s hand. You’ve most likely told yourself it will calm down.
It has not.
Tennis elbow - clinically known as lateral epicondylitis or, more precisely, lateral elbow tendinopathy - is one of the most common reasons people in Karachi see a physiotherapist. The name misleads almost everyone into thinking it is a sports injury. It is not - or at least, not usually. A 2025 comprehensive review published in the Journal of Pioneering Medical Sciences confirmed that the majority of people diagnosed with this condition are not athletes. They are desk workers, homemakers, drivers, electricians, and people who use tools - anyone doing repetitive gripping and wrist-loading work over sustained periods.
The problem with this condition is that it doesn’t heal like a muscle pull or bruise. A 2026 evidence review in JMIR Rehabilitation found that progressive loading and physiotherapy-directed strengthening remain the cornerstone of durable recovery - not rest alone. While rest and waiting can help lessen pain in the short term, without rebuilding the tendon’s load tolerance, most people end up back at square one the moment they return to normal activity. That cycle can run for months, sometimes years.
This article explains what is actually happening in your elbow, what causes it, and what the evidence says about getting better - whether you have been dealing with it for three weeks or three years. The information provided is general health information and not personal medical advice. If you are experiencing severe, worsening, or unusual symptoms, please get a proper clinical assessment before starting any exercise program.
Symptom or Trigger | What It Suggests | What To Do Next |
Pain on the outside of the elbow when gripping, lifting, or twisting | Classic tennis elbow / lateral elbow tendinopathy, often from repeated wrist and forearm loading. | Reduce aggravating activity, start load management, and seek physiotherapy if pain persists. |
Pain that worsens with mouse use, typing, tools, or carrying bags | Repetitive forearm and wrist strain is often the trigger, even in non-athletes. | Check ergonomics, modify tasks, and avoid pushing through pain for weeks. |
Pain plus numbness, tingling, swelling, fever, or obvious trauma | May not be simple tennis elbow. Could indicate nerve, joint, or other pathology. | Get a medical assessment promptly before doing exercises or manual therapy. |
Weak grip and pain opening jars, shaking hands, or turning keys | Tendon load intolerance and reduced forearm strength are common. | Physiotherapy-led strengthening is often helpful, but red flags still need evaluation. |
Why Tennis Elbow Happens
What Tennis Elbow Actually Is
The pain on the outer side of your elbow - that sharp or burning ache when you grip something, twist your forearm, or lift even a light object - comes from the common extensor tendon. This is the structure that anchors your forearm extensor muscles to a bony point on the outer elbow called the lateral epicondyle. When that tendon is overloaded repeatedly, it develops microscopic damage that the body cannot repair fast enough.
What most people misunderstand is that this is not an inflamed tendon in the way a sprained ankle is inflamed. In every tissue study, the collagen in the tendon is disorganized, there are micro-tears and abnormal blood vessel growth within the tendon - but not the classic inflammatory cells you would expect. That is why the preferred clinical term has shifted from lateral epicondylitis (which implies active inflammation) to lateral epicondylalgia or lateral elbow tendinopathy. The distinction matters because it explains why purely anti-inflammatory approaches - ice, NSAIDs, injections - often give only temporary relief without addressing the underlying tissue problem.
Tennis elbow can affect anyone from their mid-30s to mid-50s. It affects people who cook daily, carry children, use power tools, type for hours, or drive long distances with a firm grip. Research published in JMIR Rehabilitation in 2026 notes that lateral epicondylitis affects working populations at rates of 2% to 14.5% - many times higher than the general population figure of approximately 1.3%. The dominant arm carries the load in around 75% of cases. Tennis players account for only about 5% of all cases seen in clinical practice.
Why Repetition and Grip Load Trigger It
Tendons are built to handle load. That is their job. The problem is not load itself - it is too much load, applied too often, without enough recovery time. Every time you grip a steering wheel, extend your wrist against resistance, or use a mouse for six continuous hours, your common extensor tendon experiences mechanical stress. Under normal conditions the tendon adapts. When the workload consistently exceeds what the tissue can repair, small areas of breakdown accumulate. That is the start of lateral elbow tendinopathy.
The extensor carpi radialis brevis (ECRB) - one of the forearm muscles that pulls the wrist back - is the most commonly affected structure. Its attachment angle at the lateral epicondyle exposes it to shearing forces in almost every arm movement, which is why it gets into trouble more than others. Gripping amplifies the load on it. Gripping while the wrist is extended or the elbow is partially straight makes it worse. Doing that repeatedly over days and weeks without adequate recovery is precisely how most people develop this condition.
This is not a weakness or a character flaw. It is simple tissue mathematics. Construction workers using heavy tools, homemakers kneading dough and lifting heavy pots, office workers typing and mouse-clicking for eight hours, and people carrying shopping bags from the boot of a car are all exposing the same tendon to the same cumulative stress. The mechanism is nearly identical regardless of occupation. If you have also been experiencing neck tension and shoulder stiffness from prolonged desk use, it is worth reading about how screen-heavy postures strain the upper limb and shoulder - because how the whole arm is loaded from above can influence what the elbow tendon has to absorb.
What Actually Helps Recovery
Rest alone will reduce your pain.
That is both the good news and the bad news.
Removing load from an overloaded tendon allows symptoms to settle. But the tendon does not rebuild its capacity just because you stopped using it. When you return to normal activities - and you will - the tendon will be no stronger than it was before. Pain returns, often within days. The 2025 comprehensive review in the Journal of Pioneering Medical Sciences found that eccentric strengthening exercises combined with manual therapy produced up to a 42% improvement in pain scores, along with significantly improved functional outcomes. Progressive loading - exercises that gradually increase stress on the tendon in a controlled way - is how you teach the tissue to handle load again. This is the evidence base behind physiotherapy-directed rehabilitation.
Physiotherapy for tennis elbow typically combines: activity modification (not complete rest, but smarter load management), forearm extensor strengthening starting at a tolerable level and building over weeks, manual therapy targeting the elbow and wrist, and practical education about grip posture and ergonomics. The physiotherapy at home service in Karachi offered by Sehat Door brings this structured rehabilitation directly to your home - which matters when the alternative is making repeated clinic trips with a painful arm while managing work and family commitments.
Recovery is not a straight line. On some days the tendon seems to be practically normal. Then you carry something heavier than usual and the pain spikes. That is not a setback - it is load feedback. The goal of physiotherapy is to progressively widen the window of what your tendon can tolerate, so that normal daily tasks no longer trigger pain at all. Realistic timelines are 6–12 weeks for milder cases and 3–6 months for more established tendinopathy. The earlier you address this properly, the shorter that window tends to be.

Braces, Ice, Medication, and Injections: What They Can and Cannot Do
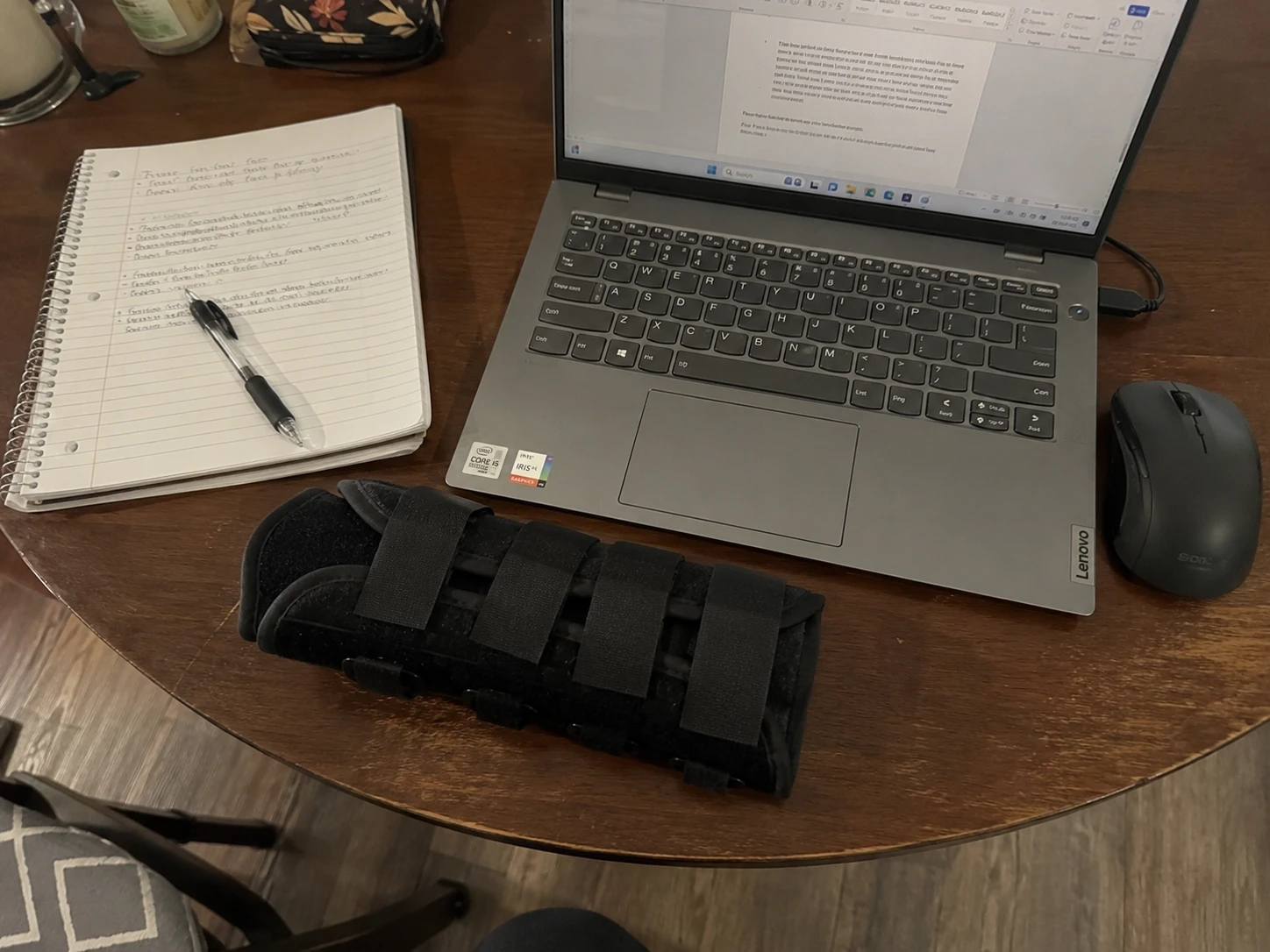
A counterforce brace - the forearm strap worn just below the elbow - reduces pain during activity by redistributing load away from the most irritated part of the tendon attachment. Used correctly, it is a useful short-term management tool. Used incorrectly, people wear it constantly for months, never progress their tendon strength, and end up dependent on it. A brace does not fix the tendon. It manages symptoms while you do the real work.
Cold packs applied for 10–15 minutes after aggravating activity can blunt post-activity pain. Over-the-counter pain relief - paracetamol or short-course NSAIDs like ibuprofen - has a role in reducing day-to-day pain levels enough to allow rehabilitation to begin. Neither ice nor medication replaces the process of loading the tendon progressively.
Corticosteroid injections can produce fast pain relief, often within one to two weeks. That short-term benefit is real. The long-term picture is different. According to 2026 evidence reviewed by CK Physio, the one-year recurrence rate after corticosteroid injection is substantially higher than after progressive loading physiotherapy, and outcomes at 12 months are worse than doing nothing. The use of injections cannot be considered wrong in itself, but should not be offered as an isolated treatment and should always be part of a wider rehabilitation program.
Platelet-rich plasma (PRP) has attracted interest as an injection option. The 2026 JMIR Rehabilitation review noted that PRP has reasonable supporting evidence as a conservative treatment - but does not clearly demonstrate superiority over other non-surgical approaches. The same principle applies: no injection replaces a structured loading program. If injections are being discussed, ask how they fit into the overall rehabilitation plan.
When Tennis Elbow Is Not Tennis Elbow
Most outer-elbow pain in people doing repetitive work is lateral elbow tendinopathy. But not all of it is. Treating the wrong condition confidently will not help and may delay appropriate care.
The following signs mean you should stop self-managing and get a proper medical assessment:
Numbness or tingling running into the hand or fingers - this may suggest posterior interosseous nerve compression or radial tunnel syndrome, which can closely mimic or coexist with tennis elbow. A 2025 paper in the Irish Journal of Medical Science specifically highlighted that posterior interosseous nerve compression is frequently overlooked in patients with refractory lateral epicondylitis.
Pain at rest or at night - tendon pain is typically load-related. Persistent pain without activity raises the possibility of inflammatory pathology or joint disease.
Obvious trauma - a fall, direct blow, or forceful sudden strain needs assessment to rule out fracture or ligament injury before any exercise is started.
Swelling, redness, warmth, or fever - these suggest possible infection or inflammatory arthritis that requires medical evaluation, not physiotherapy alone.
Sudden or severe grip weakness - reduced grip strength is common in tennis elbow, but rapid or marked loss of hand or wrist function needs urgent assessment.
Neck or shoulder symptoms accompanying the elbow pain - cervical spine nerve referral can produce lateral arm and elbow pain that is entirely separate from the tendon.
If your pain is not responding to appropriate physiotherapy after 6–8 weeks, a reassessment is warranted. The diagnosis may need revisiting. For those in Karachi, elbow pain treatment at home in Karachi through Sehat Door allows a qualified physiotherapist to assess you properly - in your own space, without the clinic trip, and without using a painful arm to navigate traffic.
What People Get Wrong About Tennis Elbow
Pushing through pain because "it will warm up." Tendons do not loosen up and stop hurting mid-session the way muscles sometimes do. Pain during activity is the tendon signaling that the load exceeds its current capacity.
Resting completely for three or four weeks, deciding the problem is gone, then returning to full activity with no strengthening plan. The tendon will fail again at the first significant load. Rest treats the symptom, not the underlying capacity deficit.
Wearing a counterforce brace every day for months without doing any forearm strengthening. The brace helps you function through pain - it does not rebuild the tendon. At some point you have to load the tissue progressively, or nothing changes permanently.
Ignoring ergonomics entirely. Mouse grip, tool handle diameter, keyboard wrist angle, and lifting technique all contribute. Most people with work-related lateral elbow tendinopathy have been doing one thing slightly wrong for a long time. Fixing it is not optional if you want to stop this recurring.
Assuming every outer-elbow pain is tennis elbow and treating it as such without proper assessment. Radial tunnel syndrome, joint pathology, referred neck pain, and inflammatory arthritis can all produce lateral elbow symptoms. Treating the wrong condition confidently is not a good plan.
Follow the Sehat Door guide if you are weighing up the difference between physiotherapy, chiropractic, and massage, the guide covers the distinctions clearly and is relevant to deciding which type of care is right for your situation.
Rapid-Fire Clinical FAQs
What causes tennis elbow in non-athletes?
Repetitive gripping, wrist extension, and forearm loading in any daily activity can overload the common extensor tendon - desk work, cooking, tool use, driving, and childcare all qualify. See a physiotherapist if pain has persisted for more than two to three weeks despite reducing activity.
How long does tennis elbow take to heal?
Mild cases with appropriate load management may settle within 6–12 weeks. More established tendinopathy often requires 3–6 months of structured rehabilitation. If you have been managing it for more than three months without meaningful improvement, a proper clinical assessment is overdue.
Can physiotherapy fix tennis elbow without injections or surgery?
For the large majority of people, yes. Progressive loading-based physiotherapy is the most evidence-supported treatment for lateral elbow tendinopathy, with durable outcomes at 12 months that outperform injections alone. Surgery is considered only in a small minority of chronic, refractory cases.
Is a tennis elbow brace actually useful?
A counterforce forearm strap can reduce pain during activity by redistributing load - useful as a short-term tool while you rehabilitate. It is not a treatment on its own. Extended reliance on a brace without any strengthening work is one of the most common reasons people plateau and do not fully recover.
Should I stop all exercise if I have tennis elbow?
No. Complete rest weakens the tendon further and does not address the capacity problem. The goal is to modify activity to a level that does not aggravate pain, then gradually increase load under physiotherapy guidance. Continuing tolerable activity is generally better than stopping everything.
When should I see a doctor instead of waiting it out?
If your pain is severe, involves numbness or tingling, came from a trauma, is accompanied by swelling, redness, warmth, or fever, or has not improved at all after four to six weeks of appropriate self-management, see a doctor or physiotherapist promptly. Do not wait for the pain to become chronic.
Can tennis elbow be confused with nerve pain or arthritis?
Yes. Radial tunnel syndrome, posterior interosseous nerve compression, and cervical nerve root referral can all produce pain in the lateral elbow and forearm that closely mimics tendon pain. Inflammatory arthritis affecting the elbow joint is another possibility. A qualified clinician can differentiate these - do not assume the diagnosis without assessment.
Untreated lateral elbow tendinopathy rarely resolves on its own when the person keeps doing the activity that caused it. The tendon develops a tolerance problem: loads that should feel normal start triggering pain because the tissue never regained its capacity. Grip strength declines quietly. The person accommodates - using the other hand, avoiding certain movements, stepping back from sport or hobbies they enjoy. Over months, what began as a minor ache can significantly interfere with work output, domestic activity, and physical wellbeing. The window to address this efficiently is early, with the right loading strategy and professional guidance, not another few weeks of hoping it will settle.
Disclaimer: This article is written for general health education purposes only and does not constitute a personal diagnosis, medical advice, or a treatment recommendation. If you are experiencing persistent elbow pain, numbness, significant weakness, or any of the red flag symptoms described above, please consult a qualified healthcare professional before starting any exercise or rehabilitation program.

Dr. Aleena PT
A Physiotherapy Doctor (DPT) from Jinnah Sindh Medical University, focused on musculoskeletal rehabilitation, evidence-based patient care, pain management, mobility improvement, and recovery support.